We have seen in the previous article the origin of Hua Tuo jia ji, these treatment points which are widely used in Shiatsu. We are going to deepen our understanding of them, since, even if they do not have the same action as the ones located on the 1st chain of the Urinary Bladder, they are still in a sense interrelated to them. Let’s take a closer look at these points by following the anatomical path.
As a reminder, we have said that this family of points is located 0.5 cun from the dorsal apophysis of the vertebrae, i.e., one thumb’s distance from the Urinary Bladder 1st line. This distance by itself should not make us confuse them. But it is the anatomy that will allow us to better understand their location.
A little anatomy has never hurt.
All along the spine, between each vertebra, there is a nerve exit called the intervertebral foramen. This is where spinal nerves exit, in other words, they emerge from the spine. These nerves exit directly from the spinal cord contained and protected by the vertebrae. There are 28 spinal nerves on both sides. But depending on where they are located, they are formed differently.
For the cervical and sacral nerves, as well as the tailbone nerve, they will quickly fuse together to form a nervous plexus. A nerve plexus is a place where several nerves meet, interconnect and form an anastomosis with tissues or organ(s). Anastomosis is the equivalent of the word “stapled”, so it is a gathering of several tissues, nerves, but this phenomenon is particularly common in the blood system.
Before going any further, it is also important to know that a spinal nerve quickly divides into many branches. The ventral or anterior branch and the dorsal or posterior branch. Only the ventral branch dives into the tissues and fuses into a plexus.
The nerve plexuses from the spine
We have many plexuses in the human body. Let’s see only those that come from the spinal nerves.
1. The cervical plexus: the nerves C1 to C4 fuse to form a command center that will actuate most of the posterior muscles of the neck. They also innervate the skin of the lateral and lower half of the head, the front of the neck and a small part of the shoulders and the front of the thorax. Finally, it also plays a role in the downward function of the diaphragm, and thus allows breathing, which is no small matter.
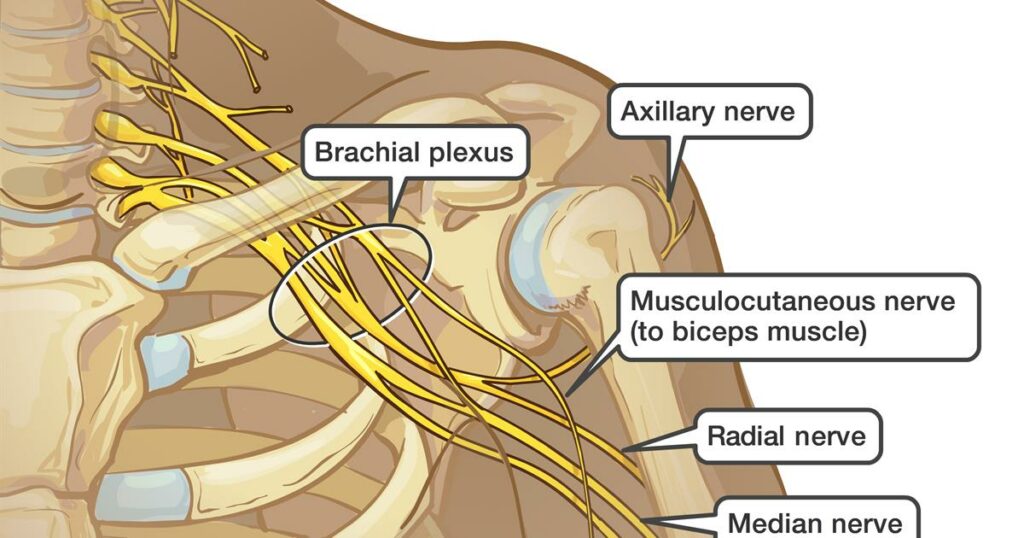
2. The brachial plexus: located at the back of the axillary region and at the base of the neck, this plexus unites the C5 to C8 nerves (note that there are 7 cervical nerves, but 8 cervical nerves), as well as that of T1. The brachial plexus is composed of three trunks. In the first trunk it is the fusion of C5 and C6, in the second C7 is all alone and in the third it is the fusion of C8 to T1. They control the scapula, the serratus anterior muscle, the scalene muscles which are crucial for the neck’s mobility, the 1st intercostal nerve in T1, and finally the skin and muscles of the pectorals, the thoracic cage and the arms. But to be able to control the hands, the three trunks divide again and re-merge in an anastomosis to give all the nerves (called terminal nerves) of the hand: the musculocutaneous, median, ulnar, radial, and axillary nerves which allow all the movements and all the sensitivities of the arm and the hand.
3. The lumbar plexus: this is where it all starts to become interesting. We went from the upper body directly to the lower part to find the next nervous plexus. This leads us to think about the thoracic nerves that we will see later… Again, these are the ventral branches that merge, from L1 to L4 with a branch from T12 to give an easy twist. They serve to innerve the abdominal wall, the genital organs, and the lower limbs. On the way to the toes, they obviously undergo some changes which generate terminal nerves: the obturator nerve (for all the adductors and the pectineus muscle) and the femoral nerve (also pectineus, iliacus, quadriceps) … Let’s stop here.
4. The sacral plexus: last plexus coming from the spinal nerves, it gathers the nerves from L5 to S4, with an additional branch coming from L4. This allows us to understand that all plexuses are communicating with each other thanks to a connecting nerve. In this case it is the innervation of the gluteal muscles, quadratus femoris and the internal muscle obturator. The terminal nerves which are the well-known sciatic nerve, the common fibula nerve and the tibial nerve.
5. Be aware that there are other nerve plexuses that will not be discussed here in detail: the pudendal or “shameful” plexus (S2 to S4) for the rectus muscles, the coccygeal plexus (S4 to Cx1) innervates the perineum.
What is noteworthy here is that the upper and lower plexuses allow the ventral spinal nerves to be mutualized to serve as actual command centers for large parts of the body.
It is worth mentioning that these are mainly motor nerves, therefore connected to the ortho-sympathetic system. Indeed, apart from a specific disorder, your arm will not move without your willingness, nor your legs or your neck. Only the diaphragm has a double connection that allows you to let your breathing go in automatic mode or accelerate or slow down your breathing rate. The diaphragm is therefore a member of the two most prominent nervous clubs: the ortho and the parasympathetic.
Finally, it should be noted that none of these nerves are part of the historical Hua Tuo jia ji points of which there are 17. They were added later by modern acupuncturists. Why is that? Probably because the famous physician Hua Tuo could not unravel the complexity of the anastomoses and terminal branches with the tools of his time. Who knows? However, it was much easier for him to follow the thoracic nerves.
What about the thoracic nerves?
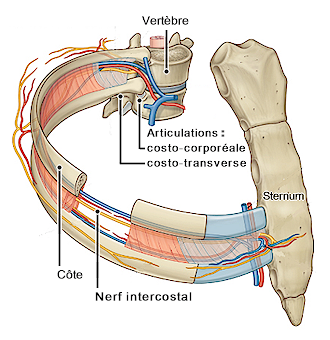
The thoracic nerves have chosen to operate differently. Indeed, they do not merge into a plexus. There are as many intercostal nerves as there are ribs, 11 pairs in total. However, the first 6 do not leave the intercostal spaces and run horizontally. On the other hand, the next 7 do the same thing and then run diagonally (forward and downward) towards the abdominal and lateral wall. As an anatomical landmark, note that the T11 nerve ends below the navel.
The common point of the thoracic nerves is to irrigate the intercostal muscles, the subcostals and the rib elevators. Those of the first team (from T1 to T6) also innervate the serratus muscles, the straight muscles and the obliques, which is always good to know when trying to release muscular tension in the back. No need to perform the whole Hua Tuo chain, these are enough. Those of the second group (from T7 to T11) do the same, but also stimulate the abdomen.
Some of you will probably be disappointed not to see any relationship between the nerves and the organs, which could undermine the theory of Yu or Bei Shu points. Because yes, all nerves are connected to muscles, and therefore to the musculoskeletal system which is itself driven by the orthosympathetic system. But wait! The best is yet to come.
The sympathetic chain
Hua Tuo, who lived a century AD, was not mistaken. The 17 points he identified and named Jia ji belong to the sympathetic trunk and not to the intercostal nerves. At the outlet of each spinal nerve, there is a nerve ganglion on the transverse apophysis and very close to the dorsal apophysis (0.5 cun away). There are 22 on each side (a little more than the classical points, hence the modern doctors desire of expand them) and they are split into:
- 3 cervical
- 11 thoracic
- 4 lumbar
- 4 sacral
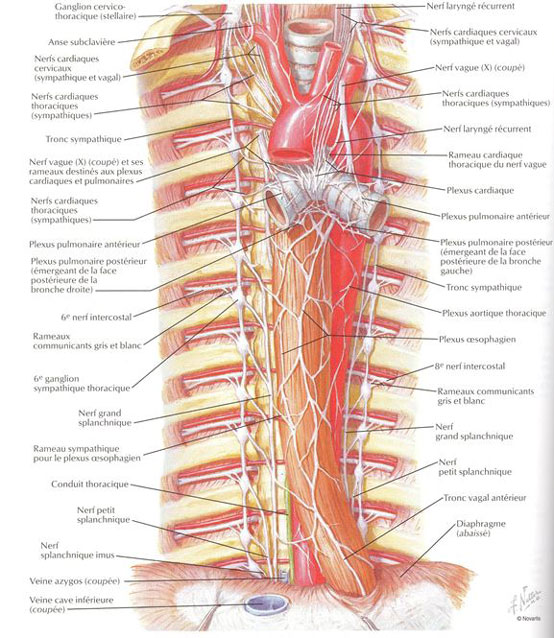
This is more like something we know. Even better, all these ganglia are connected to each other by a nerve pathway of the autonomic (parasympathetic) nervous system. Therefore, all ganglia form a chain along the vertebral body exactly where the Hua Tuo jia ji are located. Conclusion: each ganglion is in connection with the whole spinal nervous system.
But here is the best part: these ganglia send messages not only to the intercostal nerves (thus to the locomotor system), but also (via the spinal trunk) to the splanchnic nerves. These nerves meet in the frontal part of the spine and the aorta to form new plexuses which are all related to the organs. These nerves will form additional plexuses that are all innervated by fibers from the sympathetic trunk as well as parasympathetic from the vagus nerve and the pelvic splanchnic. Below is the list:
- The celiac (or solar)
- The superior, intermediate, and inferior mesenteric
- The superior and inferior hypogastric
Distinguishing between the Hua Tuo jia ji and the Bei Shu points
I know it’s complicated, and I must admit that I have thought about this question for a long time without finding a satisfying answer apart from the difference in location of course. So, when you don’t know, you ask people who are more advanced than you.
I first discussed this with Bernard Bouheret [i], a well-known Parisian Shiatsu teacher. Here is what he told me:
“Hua Tuo points are located on the vertebral body 0.5 cun from the dorsal apophysis, they are definitely easier to pressure in Shiatsu, because their structure is stable. On the other hand, the Bei Shu points, which communicate with the muscles via the intercostal nervous system, are located on the 1st chain of the Urinary Bladder meridian at the joint of the transverse apophysis and the rib (1.5 cun away). And since it is a articulation, it is not as stable to pressure. An acupuncturist will not be concerned about this difference, but a shiatsushi must take this into account.
This is now clearer. But do we touch the nerve directly when we press a Bei Shu? I asked Alexandre Noël, who is an anatomy lecturer at the Paris School of Shiatsu Therapeutics [ii], for clarification. ii] He answered me, amongst other things, that:
“The posterior (or dorsal) sensitive root of the nerve is hidden behind the vertebral blade. So, it is very unlikely that we will touch it directly by pressing on a Bei Shu, but rather indirectly. Thus, we will have an impact via the Shiatsu pressure and thus on the organ connected to it. Let’s remember that in this article we are speaking about anatomy and not about energy.
But as I like to delve deeper, I turned to Jean-Sylvain Prot [iii], a professor of acupuncture who is very interesting in his writings as well as in his lectures, particularly for his advocacy of a truly classical Chinese medicine, far from what we know from TCM books. In one of his articles entitled “Dorsal Shu points and anterior Mu points”, there is some brain scratching powder that forces us to go further in our understanding of these points. Here is the extract from his article that raises the question:
“These points [the Bei Shu] are all subcutaneous. They are located vertically to the vertebrae without any direct nervous connection with them, because the innervation of the dermis does not correspond to that of the underlying vertebra, except for the first dorsal ones.
The vertebra simply serves as a marker for the projection of a visceral dysfunction to the skin.
The relationship can nevertheless become structural. Indeed, the dysfunction of the Bei Shu region on the surface, if it persists, will progressively modify the connective tissue, become a fibrosis and affect the vertebra in depth.
This relationship between the surface and the depth thus gives all the value to the techniques on the fascia’s used in osteopathy, which, based on the subcutaneous zone in relation with the vertebrae, considers a regulation of the dysfunctions which affect the organs.
From the surface to the deep layers, it is possible to achieve a harmonization between the spinal structure and the visceral function.
The Bei Shu points would therefore also be areas of projection of the organs at the cutaneous level…. I became further intrigued and discussed this directly with the author, who told me:
“The work of Dr. Henri Jarricot [iv] has made it possible to establish, at the thoraco-abdominal level, reliable relations between the organs and the cutaneous territories.
When an organ is dysfunctional, it expresses at the skin level a dermalgia (thickening of the dermis and pain detected on palpation) on a dermatome.
This objectification of skin thickening, and exposed pain is a simple and marvelous mean to perceive the dysfunctions projected to the dermis by the viscera.
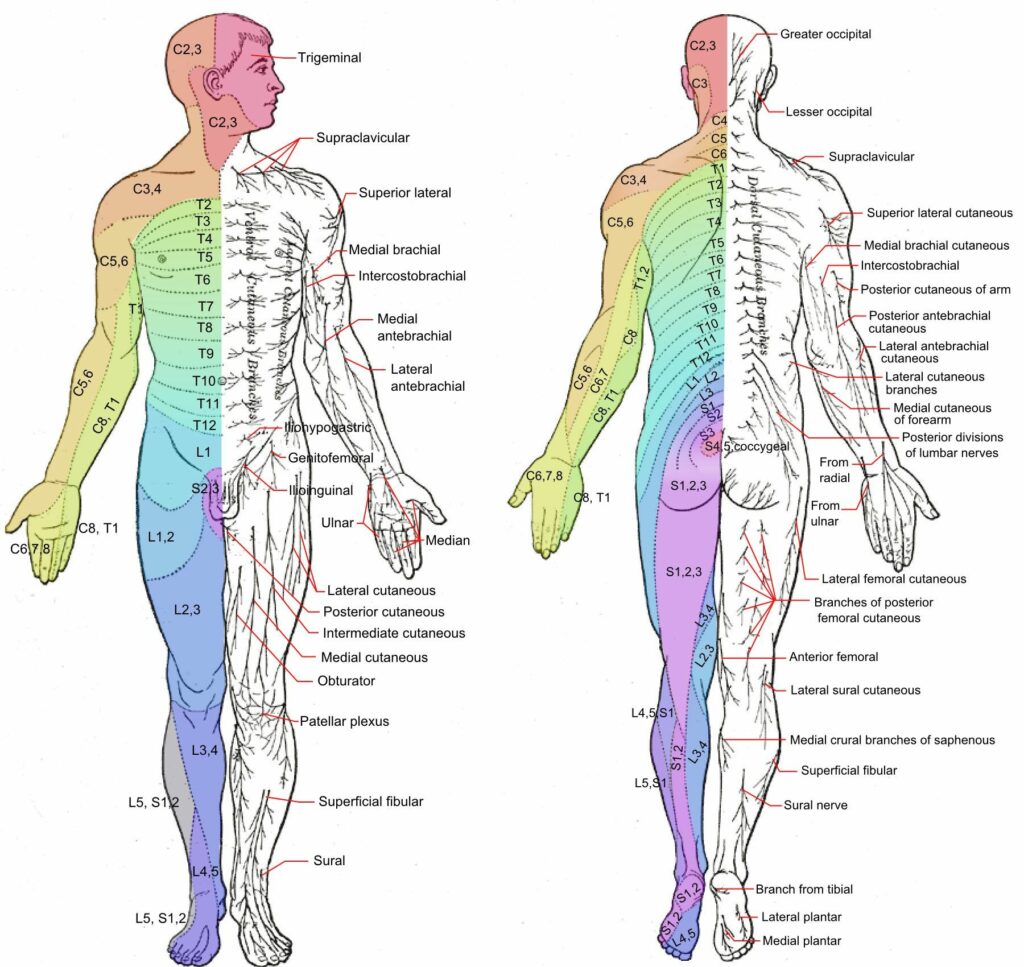
The dermatome is described as the cutaneous area that is dependent of a posterior spinal nerve root; it is a solely a sensorial zone.
The sympathetic innervation of the viscera comes from the nerve roots of the vertebrae from T2 to L2.
The dermatomes, related to the vertebrae from T2 to L2, are distributed on the trunk from the back to the front, oblique at the bottom and in the belt.
At the first level of the thoracic vertebrae, there is concordance between the vertebrae and the dermatomes, but the more one goes down the spine, the more one observes a shift.
The bottom of the T10 dermatome is defined horizontally at the vertical of the L1/L2 vertebrae. The T11 dermatome ends up horizontally at the vertical of the L3/L4 vertebrae. The T12 dermatome follows the iliac crests and ends horizontally at the vertical of the L5/S1 joint space.
The Bei Shu points establish a relationship between the subcutaneous tissue and the organs. They indicate on the surface, in line with a vertebra, the quality of the organ located deep down. These points are subcutaneous, on the surface. They are vertical to the vertebrae without any direct nervous connection with them because the innervation of the skin does not correspond to that of the underlying vertebra, except for the first dorsal ones.
We see with the thoraco-abdominal dermalgia of Dr Henri Jarricot, the accurate relationship that exists between the vertebrae and the projection of the organs on the dermis. For the Shu points, the vertebra serves as a reference point for the projection of an organ dysfunction onto the dermis.
Conclusion
When one seeks, one finds! And this sometimes takes us out of our comfort zone, and this is precisely what is exciting about this endless study of the body and Oriental medicine! Here we are with a very exciting and somewhat new vision (at least for me who is now writing to you) of Bei Shu. But at least, one thing is crystal clear: Bei Shu and Hua Tuo jia ji have nothing to do with each other even if both have an influence on the organs.
Good practice!
Author

- Bosnia – 5-6 April 25: 1st Balkan Shiatsu Summit in Sarajevo - 31 January 2025
- Austria – 19-21 Sept. 25: Shiatsu Summit in Vienna – chronic fatigue, burnout & depression - 19 December 2024
- Terésa Hadland interview: Shiatsu at core - 25 November 2024
- Book review: “Another self” by Cindy Engel - 30 September 2024
- Austria – 24-26 Oct. 25: Master Class in Vienna – Shiatsu and martial arts - 20 August 2024
- France – Lembrun Summer Intensive Course – July 6 to 12, 2025: Digestive System Disorders, Advanced Organ Anatomy, and Nutrition - 4 August 2024
Translator

Fascinated by Energy and everything that is related to the development of the Human Being, he started his career as an Energy Therapist before training with Florent Dagobert in the school "La Voie Shiatsu" as a Shiatsu Specialist (RNCP title).
Francois-remy continues to integrate various techniques through additional training and reading, which is one of his passions.